

How Mandibular Advancement Devices Work: A Clear Guide to This Proven Sleep Apnea Solution
If CPAP feels like too much, a mandibular advancement device may be the evidence-backed alternative to your sleep has been waiting for.
Everything You Need to Know About Mandibular Advancement Devices
What exactly is a mandibular advancement device?
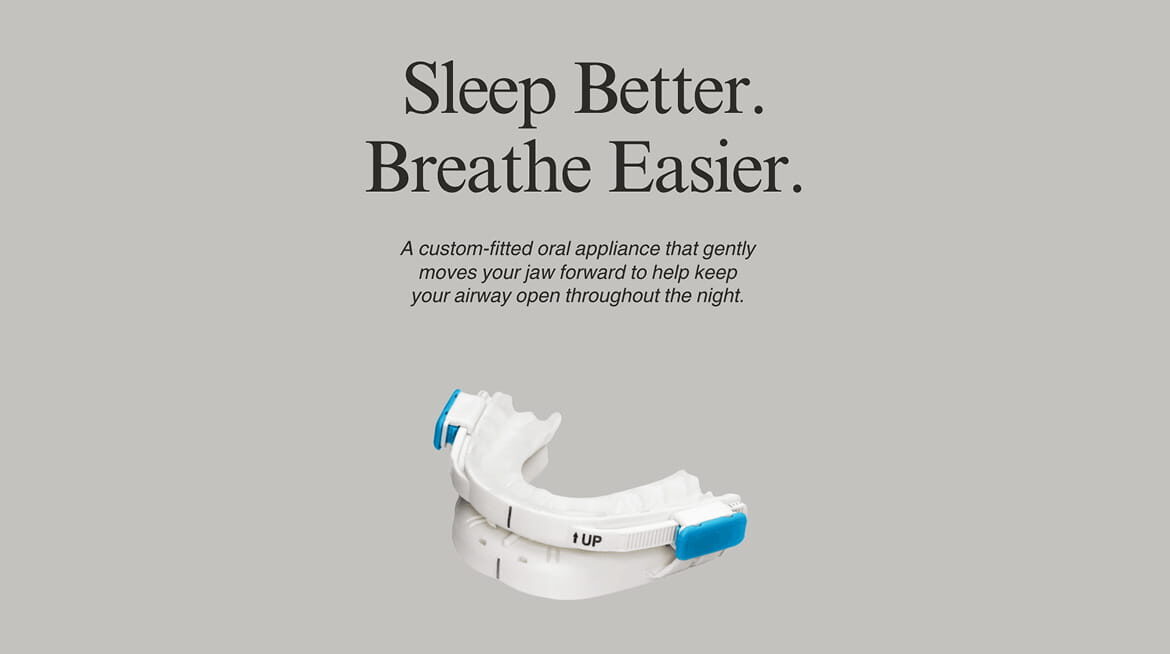
A mandibular advancement device (MAD) is a custom-fitted oral appliance worn during sleep that gently repositions the lower jaw (mandible) slightly forward and downward. This forward positioning tightens the soft tissues and muscles of the upper airway, reducing the likelihood of collapse or vibration that causes snoring and obstructive sleep apnea (OSA).
In appearance, a MAD resembles a sports mouthguard, though it is considerably more precisely engineered. It consists of two connected trays, one fitting over the upper teeth and one over the lower, with an adjustable mechanism that controls the degree of jaw advancement (Ramar et al., 2015).
MADs are not a one-size-fits-all solution. Devices prescribed and fitted by a trained dentist or sleep specialist are custom-fabricated to the patient’s bite and anatomy, which significantly improves both comfort and clinical effectiveness compared to over-the-counter alternatives.
What is actually happening in the airway when a MAD is worn?
To understand how a MAD works, it helps to understand why the airway collapses in the first place. During sleep, the muscles supporting the tongue, soft palate, and throat naturally relax. In people with OSA or habitual snoring, this relaxation is pronounced enough that the airway narrows significantly or closes altogether. The result is interrupted airflow, oxygen desaturation, and the repeated arousal cycles that fragment sleep.
When a MAD advances the lower jaw forward, it pulls the tongue and the attached soft tissue structures away from the back of the throat. This mechanical displacement increases the cross-sectional area of the pharyngeal airway and reduces its tendency to collapse under the negative pressure of inhalation (Ferguson et al., 2006).
Imaging studies using MRI and CT scans have confirmed that MAD therapy produces measurable, consistent enlargement of the upper airway in multiple anatomical dimensions, particularly in the lateral (side-to-side) direction (Sutherland et al., 2014).
Who is a good candidate for a mandibular advancement device?
MADs are clinically indicated across a broad range of patients, though they are most effective in specific profiles.
The strongest candidates include:
- Adults with mild-to-moderate OSA (apnea-hypopnea index of 5 to 30 events per hour)
- Patients with primary snoring without significant apnea
- CPAP-intolerant patients who have moderate-to-severe OSA but cannot or will not use
continuous positive airway pressure consistently - Patients whose OSA is positional (worsening when lying on the back)
- Younger patients with less anatomically compromised airways
Clinical practice guidelines from the American Academy of Sleep Medicine and the American Academy of Dental Sleep Medicine recommend MAD as a first-line treatment for mild-to-moderate OSA and as an appropriate CPAP alternative for severe OSA when CPAP adherence is poor (Ramar et al., 2015).
Patients with significant temporomandibular joint (TMJ) disorders, insufficient healthy teeth, or severe periodontal disease may not be suitable candidates and require individual assessment.
How effective are mandibular advancement devices compared to CPAP?
This is the question most patients want answered, and the evidence provides a nuanced but encouraging picture.
CPAP remains the most effective treatment for reducing the apnea-hypopnea index (AHI) in controlled settings. However, treatment effectiveness in the real world depends heavily on how consistently a therapy is actually used. MADs consistently outperform CPAP on adherence metrics, with patients wearing their devices significantly more hours per night on average (Sutherland et al., 2014).
A landmark randomized crossover trial published in the American Journal of Respiratory and Critical Care Medicine found that while CPAP produced greater reductions in AHI under laboratory conditions, MAD and CPAP resulted in comparable improvements in daytime sleepiness, quality of life, and blood pressure when measured across real-world use (Engleman
et al., 2002).
A systematic review and meta-analysis further confirmed that MADs significantly reduce AHI, oxygen desaturation index, and subjective sleepiness, with the greatest benefit seen in patients with mild-to-moderate disease severity (Lim et al., 2006).
The practical conclusion: a MAD worn consistently every night often delivers better health outcomes than a CPAP machine used only intermittently.
How is a mandibular advancement device properly fitted and adjusted?
The fitting process is more involved than simply taking an impression of the teeth, and this precision is what separates clinically effective devices from over-the-counter products. A qualified dentist with training in dental sleep medicine will typically conduct a comprehensive oral examination to assess teeth, gums, bite, and jaw joint health. Dental impressions or digital scans are taken to fabricate a device custom-molded to the patient’s exact anatomy.
Once the device is delivered, the critical process of titration begins. Titration refers to the gradual, incremental advancement of the lower jaw in small steps (usually 0.25 to 0.5 mm at a time) until the optimal therapeutic position is reached, meaning the position at which snoring and apnea events are sufficiently reduced with acceptable comfort (Tsuda et al., 2010). This titration process may take several weeks to months. Follow-up sleep testing is typically conducted after titration is complete to objectively verify that the device is achieving its intended clinical effect.
What side effects should patients expect, and how are they managed?
MAD therapy is generally well-tolerated, but side effects are common, particularly in the early weeks of use. Most are manageable and resolve with proper adjustment.
The most frequently reported side effects include:
Jaw soreness and muscle tenderness are the most common early complaints. These typically diminish as the jaw adapts to the new position over the first few weeks. Morning jaw exercises and gradual titration minimize discomfort (Marklund et al., 2004).
Excessive salivation or dry mouth occurs as the oral environment adjusts. Both effects are generally temporary and self-limiting.
Tooth discomfort and minor bite changes are reported by some patients, particularly in the morning after removing the device. A brief morning re-alignment exercise, where the patient gently bites together on a soft surface, helps restore normal occlusion quickly (Almeida et al., 2006).
Temporomandibular joint discomfort is a more significant concern in susceptible individuals. Regular monitoring by the prescribing dentist is important to catch and address any joint-related issues early.
Long-term tooth movement is a less common but documented concern with extended MAD use, reinforcing the importance of ongoing dental supervision rather than unsupervised, indefinite Self-treatment.
How does a mandibular advancement device compare to surgery for sleep apnea?
For many patients, MAD therapy occupies a valuable middle ground between conservative measures and surgical intervention. Surgical options for OSA, such as uvulopalatopharyngoplasty (UPPP) or maxillomandibular advancement (MMA) surgery, carry inherent procedural risks, require recovery time, and produce variable outcomes that are difficult to predict preoperatively. Success rates for soft tissue surgeries like UPPP are inconsistent, with long-term cure rates often below 50% in unselected populations (Caples et al., 2010).
MAD therapy, by contrast, is reversible, non-invasive, and adjustable. If a patient’s anatomy or disease severity changes over time, the device can be modified or replaced without any permanent consequences.
That said, surgical approaches such as MMA, which physically enlarges the skeletal framework of the airway, do produce more dramatic and durable anatomical changes than MAD therapy.
For patients with severe skeletal abnormalities driving their OSA, surgery may ultimately be the more effective long-term solution. A thorough evaluation by both a sleep physician and an oral and maxillofacial surgeon helps determine the most appropriate path.
What should someone expect in terms of long-term use and outcomes?
MAD therapy is a long-term commitment rather than a short-term intervention, and outcomes tend to improve as the device is properly titrated and the patient adapts.
Long-term adherence rates for MADs are favorable. Studies tracking patients over five or more years report that the majority of patients continue using their devices nightly and report sustained improvements in sleep quality, snoring reduction, and daytime functioning (Marklund et al., 2004).
Periodic reassessment is important. OSA can change in severity over time with weight fluctuations, aging, or anatomical changes. Annual follow-up with the treating dentist and periodic sleep testing help ensure the device continues to perform at the required therapeutic Level.
Devices typically require replacement every three to five years due to normal wear, and some patients require bite adjustments or new fabrications as their oral anatomy changes over time. For patients who find the right device and complete a proper titration process, the outcome is frequently transformative: quieter nights, deeper sleep, and a meaningful reduction in the health risks that untreated sleep apnea carries over a lifetime.
Ready to Explore Whether a MAD Is Right for You?
A mandibular advancement device is not a universal solution, but for the right patient, it is a clinically validated, comfortable, and highly effective path to better sleep and better health. If you have been diagnosed with mild-to-moderate sleep apnea, struggle with CPAP compliance, or are simply looking for an alternative to a mask and machine, speaking with a dentist trained in dental sleep medicine is a logical and worthwhile next step. Better sleep is not out of reach. Sometimes, it just takes the right fit.

